






Fifteen years ago, this 44-year-old, 300-plus-pound patient presented to our clinic ambulating on a walker seeking alternative treatment to knee replacement surgery. After spending one month in a hospital because of debilitating knee pain and failing traditional therapy, he was told he needed knee replacement surgery.
Patient has had three knee surgeries
Initial Autologous treatments:
Since 2011, the patient has been treated four times over the years, and his last treatment was on 12/16/ 25. He has not had a knee replacement, and he has lost 80 lbs. because he is free of debilitating pain and can exercise.

The patient has only had advanced autologous (same donor, same recipient) cellular injections of Cytokine Rich Plasma CRP, which is a more purified method of Platelet Rich Plasma devoid of RBCs and WBCs and higher levels of growth factors. See Fig. 2 below
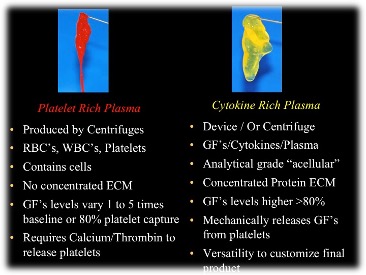
Those who are experienced in regenerative treatments understand that it takes a combination of “regenerative proteins” from the platelets and a “scaffold” to hold the proteins in the treatment area.
The “scaffold is similar to rebar”, so the denser the scaffold, the longer it will take the body to assimilate it; therefore, the entrapped regenerative proteins stay in the treatment longer to heal and regenerate. See Fig. 3 for a comparison.
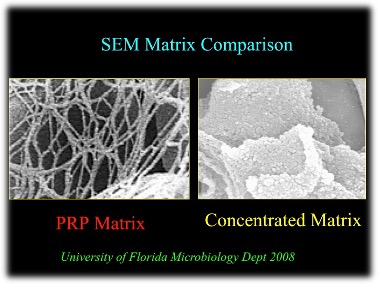
This is a comparison of the CRP natural protein scaffold on the right and the scaffold in PRP. Our CRP scaffold is concentrated from the serum of your blood, made of fibronectin, vitronectin, and osteonectin, all of your own cells.
Our process produces A2M; PRP does not!
The A2M (Alpha-2-macroglobulin) is a large plasma protein present in blood and synovial (joint) fluid. It acts as a broad-spectrum protease inhibitor-essentially a molecular “trap” for enzymes that break down tissue.
Bottom line, the A2M modifies (slows down) osteoarthritis, and this is why we have seen many patients put off knee replacement for years. These treatments are not stem cells, but we are harnessing your own cells to regenerate the damaged cells.
Stem cells and Exosomes can be added to this structure, and now you have your own regenerative cells, a protein scaffold, and signaling cells.